
Non-traumatic intramural hematomas in patients on anticoagulant therapy
Non-traumatic intramural hematomas in patients on anticoagulant therapy: Report of three cases and overview of the literature
Introduction
Non-traumatic intramural hematoma in the gastrointestinal tract is a rare event that could have diverse clinical presentation. The small intestine is the site of predilection to this condition. Intestinal obstruction is the main presentation. Various degrees of acute abdominal pain with peritoneal signs would make a cumbersome diagnosis.
Case reports
Retrospective review of the surgical emergency admissions database was conducted back to 1994. A literature overview was conducted. Three cases were retrieved and presented in this manuscript. More than 20 reports, with acute abdominal pain as a main presentation, were found in the literature.
Discussion
Complete history taking is mandatory not to miss such an uncommon complication. The INR level should be asked for in every case on oral anticoagulant presenting with acute abdominal pain. CT scan is the main diagnostic tool. Conservative management is the standard therapeutic approach.

Non-traumatic intramural hematoma of the gastrointestinal tract complicating anticoagulant therapy is an uncommon event. It is mainly associated with warfarin and less commonly reported with other anticoagulants. Warfarin doses vary considerably between patients, with Factor VII polymorphism thought to be mainly responsible, although ambient temperature plays a role as well. However, not all variabilities are explained by these and as of yet the process is not fully understood. The high ambient temperature in Kuwait, similar to many parts in Africa, may have likely contributed to the exaggerated response to warfarin seen in these three cases.
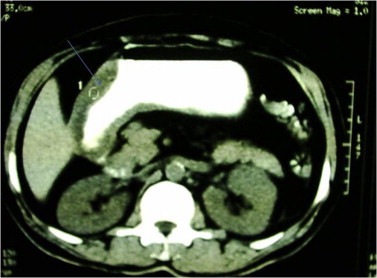
Intramural hematomas of the gastrointestinal tract can present with a multitude of signs and symptoms. Gastric mural hematomas are very rare complications of anticoagulant therapy and present mainly with upper abdominal pain and vomiting that may or may not be blood stained. Jaundice and acute pancreatitis have been reported as complications of duodenal hematomas, whilst intestinal obstruction was the main presentation for lesions occurring in the small intestine. Occasionally these lesions could present with bleeding from an orifice. Acute abdominal pain appears to be the most commonly reported symptom. All of our patients had acute abdominal pain on presentation.
Complete history taking remains of paramount importance in patients presenting with abdominal pain. As an elevated INR has been reported consistently in case reports, it should be performed on all patients on warfarin presenting with abdominal pain as it will provide a clue to the potential diagnosis. Despite endoscopy allowing direct visualization of the mucosa access is restricted in most low to middle income ECs. When available a CT provides more discrete information about not just the diagnosis, but also the extent and the mural thickness of the lesion. It is also less invasive than endoscopy, which might directly cause mucosal bleeding and ulcerations. Abdominal ultrasound can show mural thickening, but it should be borne in mind that a negative ultrasound does not rule out the intramural hematoma.
Bacterial translocation from the dysfunctional mucosa due to the accumulation of blood is associated with a leucocytosis and possibly even sepsis. WBC elevation can be over 20 thousand, which could confound the diagnosis. Higher WBC counts can be associated with more extensive hematomas.30 Lethal outcomes occur if extensive hematomas are associated with the presence of significant co-morbidities. Currently, the management includes the resuscitation and the correction of anticoagulation. We reverse warfarin induced coagulopathy with vitamin K and/or fresh frozen plasma. Prothrombin complex concentrate is widely used for this purpose in higher income settings.
The necessity for surgical intervention in these cases has diminished significantly and its role is presently reserved to those cases that do not improve using conservative measures. The extent of the mural hematoma, along with the WBCs could predict those who might require surgical intervention, however, response to resuscitation is a governing factor for decision-making. Early recognition avoids unnecessary surgical exploration.
Conclusions
An accurate detailed history is essential when assessing a patient with acute abdominal pain. Where patients on anticoagulant therapy present with abdominal pain, a coagulation profile should be considered routine. The diagnosis of a spontaneous intramural hematoma relies mainly on a detailed history and clinical examination, deranged coagulation profile and abdominal CT confirmation. The decision on how to manage the clinical condition is governed by the response to the conservative management in the first instance.
THE FULL TEXT FROM THE AFRICAN JOURNAL OF EMERGENCY MEDICINE