
Fluid resuscitation in bleeding trauma patient: are you aware of wich is the right fluid and the right strategy?
Author: Mario Rugna, MedEst118
The fluids of choice in prehospital field are, in most cases, cristalloids (Norma Saline or Lactate Ringer).
But what is the physiological impact of saline solutions when administered in large amounts (as the latest ATLS guidelines indicates) to hypotensive trauma patients?
Is aggressive Fluid resuscitation the right strategy to be pursued?
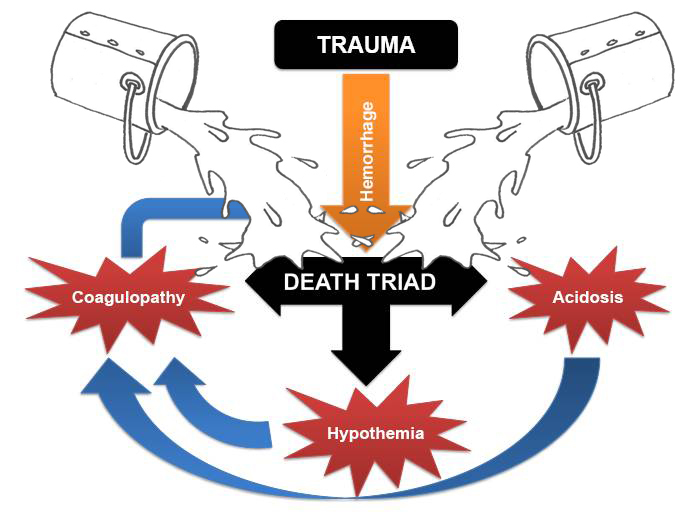
The triad of post-trauma lethal evolution is:
- Hypotermia
- Acidosis
- Coagulopathy
Aggressive fluid resuscitation with cristalloids, and saline solutions in particular, can be detrimental in many ways:
- Cristalloids tend to displace the already formed clots and improves bleeding
- Normal Saline produce hypercloremic acidosis worsening coagulation and precipitating renal and immune dysfunction
- Cristalloids diluts the coagulation factors and precipitate the coagulation system (dilution coagulopathy)
- Cristalloids rapidilly shift in intercellular space worsening SIRS process and interstitial edema (brain edema, bowel wall edema) with consequent compartment hypertension
So wich is the perfect fluid to infuse in trauma?
The perfect fluid doesn’t exists.
Balanced saline and Hypertonic saline are promisng prospective but there are still no good quality evidences about their benefit on clinical outcomes.

Colloids has no place in fluid resuscitation of trauma patients.
The fluid of choice, regarding the actual evidences and indications, is Lactate Ringer.
More than on the type of fluid the attention of researchers and clinicians is oriented on the strategy to pusue in those cases.
Hypotensive resuscitation, part of damage control resuscitation, is at the moment the strategy of choice in trauma bleeding patients.
Restrictive fluids administration is the way to achieve this goal.
The target systolic BP has to be diferentiated depending on the type of trauma
- 60–70 mmHg for penetrating trauma
- 80–90 mmHg for blunt trauma without TBI
- 100–110 mmHg for blunt trauma with TBI.
More important do not delay definitive treatment.
ASAP give blood products (PRBC, FFP etc…) to contrast post-trauma coagulopathy and send the patients in OR to fix treatable causes of bleeding
The following are a collection of un essentials resources on haemostatic resuscitation after trauma
- Current Issues in Fluid Resuscitation Following Trauma
- Fluid resuscitation in trauma patients- what should we know
- The Prospective, Observational, Multicenter, Major Trauma Transfusion (PROMMTT) Study
- Hypotensive Resuscitation
- Liberal Versus Restricted Fluid Resuscitation
- Trauma-Induced Coagulopathy
- Fluid Resuscitation for Trauma Patients: Crystalloids Versus Colloids
- Recent developments in the assessment of the multiply injured trauma patient
- Meta-analysis of high- versus low-chloride content in perioperative and critical care fluid resuscitation