
What is empyema? How do you deal with a pleural effusion?
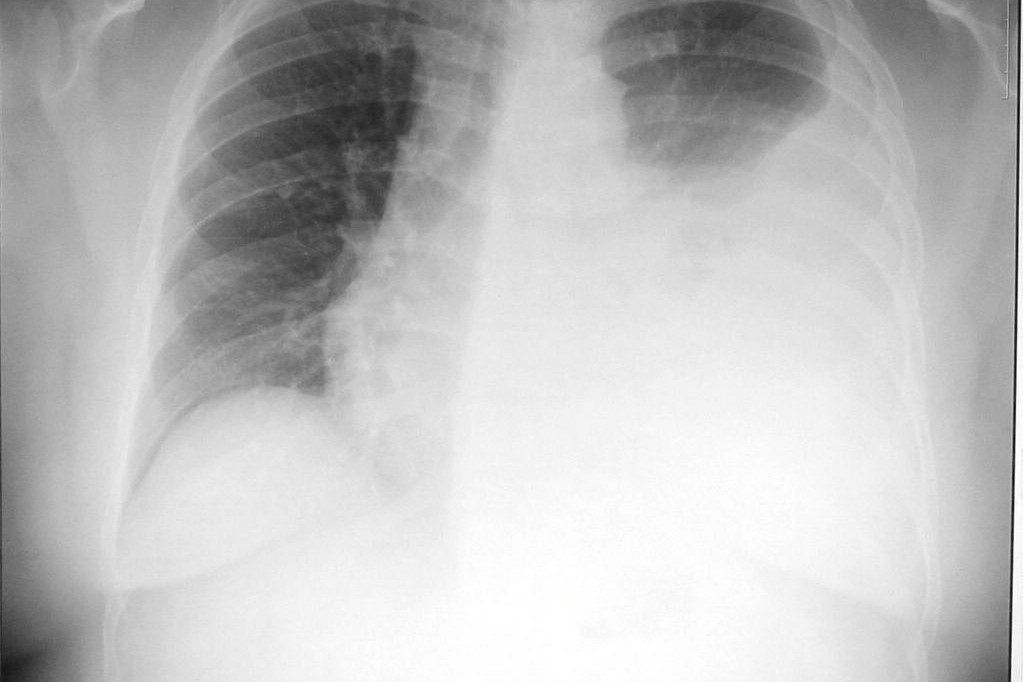
Empyema is defined as a collection of pus in the pleural space and is a form of purulent (infected), pleural effusion. Pleural effusion refers to the build-up of excess fluid between the layers of the pleura outside the lungs
What are the major substances that collect in the pleural space?
Several fluids may collect in the pleural space alongside empyema:
- Plasma ultrafiltrate, bile, urine, gastrointestinal contents, ascites (fluid build-up) chyle (a substance rich in protein, fat, and white blood cells)
- Blood
- Air
- Cells, which may manifest as pleural tumor
- Fibrosis
How do pleural effusions form?
The fluid in an empyema is filled with an infectious agent, such as tuberculosis (TB) or Staphylococcus, although many others have been identified. Most empyemas result from acute bacterial cases of pneumonia or abscesses.
Some empyemas are “culture-negative” and are sterile pleural collections that include augmented levels of inflammatory mediators, which result in systemic effects which are clinically indistinguishable from true empyema collections.
This may occur because of thoracic surgery combat trauma or occasionally, from the dissemination of extrapulmonary sites or direct spread through the diaphragm for my subphrenic abscess.
If empyemas drain into the chest wall or beyond, into soft tissue, a form of empyema called empyema necessitans, results.
In a healthy person, the pleural fluid is maintained by a balance between the oncotic and hydrostatic pressure in the lungs along with the lymphatic drainage system; any perturbations to these systems can result in a build-up of pleural fluid.
Empyemas developed in three stages.
The first is referred to as the exudative stage in which a low viscosity fluid forms.
Following this, the fibrinopurulent stage, which is a transitional phase with heavy fibrinous deposits and turbid fluid occurs.
Finally, in the organizing stage, capillary growth is seen with the lung trapping by collagen. This process typically occurs over six weeks.
Signs and diagnosis of empyema
The clinical presentation of empyema includes elevated white blood cell count, unexplained fever, and respiratory failure.
Other signs of infection include chills and chest pain.
Clinical and radiographic findings are used to diagnose empyemas. Several criteria are used to diagnose empyemas.
This includes the presence of purulent fluid which is identified based on gramme stain or culture; a white blood cell count in the pleural fluid greater than 5 x 109 cells/L and a pH below 7 or glucose level less than 40mg/ml.

CT scans can define the locations, while thoracentesis, which is the process of repeatedly drawing aliquots of fluid out of the chest with a syringe, can unearth pus, which is subsequently sent for analysis on culture.
CT scans are ideally performed with intravenous contrast to enhance the pleura.
CT scans can reveal thickening of the pleura which is present in approximately 80–100% of patients, as well as a combination of necrotic long, fluid, and air.
How should empyema be treated?
Before treating empyema, it is important to distinguish it from a long Abscess.
This can be achieved using a CT scan, in which empyemas display smooth interfaces with the lung parenchyma; in contrast, lung abscesses manifest as marginated, thick-walled circle cavities having an acute, rather than an obtuse angle of contact with the chest wall.
Long abscesses, by contrast, destroy the adjacent long as opposed to displacing it.
There are several ways in which empyemas may be treated.
The condition can cause death if left untreated, and earlier surveys have reported higher mortality rates – modern and timely therapeutic intervention can dramatically reduce death from empyema.
The management of empyema is based on evidence-based guidelines. The cold treatment is to kill the infection and remove the collection of purulent effusion.
Treatment options include:
- Antibiotics
- Chest drain – in some cases, a delay to pleural drainage is associated with increased morbidity, duration of hospital stay
- Stoma – this is an opening in the chest in which a bag is placed over this opening to collect the fluid that leaks from the empyema
- Thrombosis prophylaxis – an effective method in preventing the formation of blood clots. This is important in patients who have been admitted to the hospital due to pneumonia and/or pleural infection
Read Also:
Pain Management In Blunt Thoracic Trauma
Acute Hyperinflammatory Shock Found In British Children. New Covid-19 Pediatric Illness Symptoms?
Source:
References:
- McLoud TC, Boiselle PM (2010). Chapter 18 – The Pleura, in McLoud TC, Boiselle PM (eds.) Thoracic Radiology (Second Edition).Mosby, pp. 379–399.
- Greaves M, Brown K (2010). 1 – Imaging of the Thoracic Surgery Patient, in Saunders WB, (ed.) Medical Management of the Thoracic Surgery Patient. London: Saunders Elsevier.
- Brinckerhoff LH (2018). Chapter 82 – Thoracic Surgery for Nonneoplastic Disease, IN Alden H. Harken AH, Moore EE, (eds.) Abernathy’s Surgical Secrets (Seventh Edition). Elsevier, pp. 384–386.
- Marchiori DM (2014). Chapter 24 – Pulmonary Infections, in Clinical Imaging (Third Edition). Mosby, pp.
- Krishna R, Rudrappa M. Pleural Effusion. [Updated 2020 Oct 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448189
- teachmeanatomy.info. (2020) The Pleurae https://teachmeanatomy.info/thorax/organs/pleurae/