
ECG criteria, 3 simple rules from Ken Grauer - ECG recognize VT
A question about ectopy and aberrancy, even if of minor influence on therapy that was based on clinical presentation, was interestingly debated in ECG+ community.
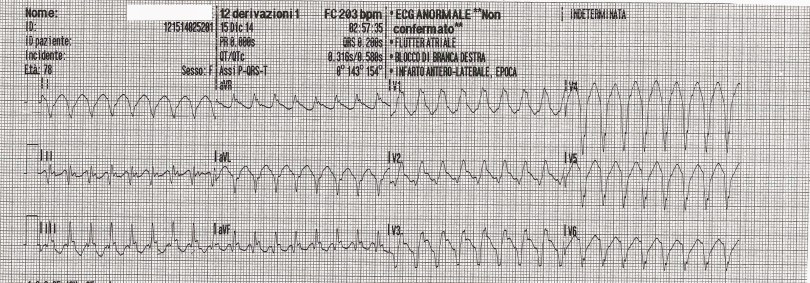
Prof. Ken Grauer and other members of the community gave the solution on why the above 12 leads ECG was, with good approximation, referrable to a VT and not to an SVT conducted with aberrancy.
Those are the ECG criteria they individuated:
- Extreme axis “northwest axis”: (neg in lead I, positive in lead aVR);
- Lead V1 is amorphous
- Lead V6 is almost all negative
- No diphasic RS complexes in any of the precordial leads
- Monophasic R-wave in lead V1(taller left “rabbit-ear”)
- Diphasic QR complexes in leads V2 and V3.
- Monophasic QS complexes in leads V4, V5, and V6.
- Josephson’s sign (notching on the nadir of S wave)
Those criteria, even if present in this case, are universally valid.



Ken Grauer, ECG master and author of many ECG books, gave us the permission to share his “3 SIMPLE Rules” to recognize VT in a simple ad accurate way.
Rule #1 Is there an extreme axis deviation during WCT?
Extreme axis deviation is easy to recognize. The QRS complex will be entirely negative in either lead I or lead aVF. The presence of extreme axis deviation during a WCT rhythm is virtually diagnostic of VT.
Rule #2 Is lead V6 all (or almost all) negative?
IF ever the QRS in lead V6 is either all negative (or almost all negative) then VT is highly likely.
Rule #3 Is the QRS during WCT “ugly”?
The “uglier” the QRS the more likely the rhythm is. VT originates from a ventricular focus outside of the conduction system. As a result, VT is more likely to be wider and far less organized (therefore “uglier”) in its conduction pattern
ECG criteria: the book
The “3 simple rules” is an extract from ACLS 2013 Arrhythmias where you can find the complete explanation and much more on arrhythmias.
Visit Ken Grauer Amazon page to find out more and discover all the amazing ECG books he wrote. They are accurate and reliable for use in many emergency situation.
I’ll include Ken’s reply in the main script of the post cause it contains some very important adjuncts and explanations. At the end of the replay, you’ll find the link to download the full text of the section regarding the WCT topic. You’ll also appreciate the perfect Ken’s Italian. I’m amazed….
I’ll make a few brief additions to what Mario wrote. RULE #1 – Remember that slight or even moderate axis deviation is of no help. The QRS complex must be ALL negative in either lead I or in lead aVF. If it is – then the rhythm is almost always VT. RULE #2 – Again, moderate negativity in lead V6 is common and means nothing. But if the QRS complex in lead V6 is either all negative or shows no more than a tiny r wave – then VT is likely. This is because such marked negativity in lead V6 implies that the impulse is moving away from the apex – and that almost always means VT. RULE #3 – Supraventricular rhythms with either preexisting bundle branch block or aberrant conduction typically resemble some form of conduction defect (ie, either RBBB, LBBB or RBBB with LAHB and/or LPHB).
However, if the QRS complex is amorphous (ie, very “ugly” and formless) – then it is much more likely to be originating from the ventricles. Occasionally, patients may have unusual forms of IVCD – so this rule is not 100% accurate – but it is a helpful supportive point in the differential diagnosis. For those wanting more complete description of the 3 Rules (and other pointers in assessing wide tachycardias) – feel free to download these Sections from my ACLS-2013-ePub
KEN GRAUER, MD is Professor Emeritus (Dept. Community Health/Family Medicine, College of Medicine, University of Florida in Gainesville). Dr. Grauer has been a leading family physician educator for over 30 years. During that time he has published (as principal author) more than 15 books and numerous study aids on the topics of ECG interpretation, cardiac arrhythmias, and ACLS. Dr. Grauer retired from practice in 2010 – however, he remains extremely active writing ECG/Arrhythmia books – making ECG videos – and actively participating in numerous on-line ECG teaching forums.
