
Pleuritis, symptoms and causes of pleural inflammation
What is the pleura? The pleura is a thin membrane that surrounds each of the two lungs. The sheets of mesothelial cells that make up the pleura have a fundamental function: to secrete a highly lubricating fluid that allows lung movement within the rib cage, reducing friction
Anatomically, a distinction is made between a visceral pleura, which lines the lungs and contains no nerve fibres, and a parietal pleura, which lines the inner surface of the thorax, the diaphragm and the mediastinum and instead contains sensitive fibres.
The two sheets are separated by a cavity that contains 5 to 10 ml of fluid, with the aforementioned lubricating functions.
The fluid is not static, but subject to continuous turnover: produced by the parietal pleura, it is reabsorbed by lymphatic capillaries located mainly at the lower diaphragmatic and mediastinal levels.
When the hydrostatic pressure in the pleural cavity increases or when the oncotic pressure (the one caused by the normal presence of proteins in the pleural fluid) decreases, there is an increase in the fluid itself, low in proteins, which is called transudate and which characterises non-infectious pleural diseases.
On the other hand, when the lymph capillaries are obstructed or secrete fluid themselves, the increase in volume of the protein-rich pleural fluid is called exudate, as occurs in all conditions of inflammation and infection.
By aspiration of the pleural fluid (thoracentesis), the fundamental differences between these two types of fluid production can be observed, which are:
- transudate = protein 60 mg/dl
- exudate = protein > 3 g/dl and glucose
What is pleuritis
Having made this anatomo-physiological premise, it is necessary to specify that the word pleuritis refers to an inflammatory condition of the pleural serosa caused by various factors, which must be distinguished from non-inflammatory pleural effusions.
The presence of a transudate (without inflammation) is almost always the consequence of three chronic diseases
- congestive heart failure
- liver cirrhosis;
- renal failure from nephrotic syndrome.
On the other hand, when we speak of pleurisy, we refer to the presence of an exudate, due in most cases to infection.
In this case, one speaks more appropriately of a para-pneumonic effusion, since pleurisy is contemporaneous or subsequent to pneumonia or a lung abscess.
If the effusion is simple, it can be reabsorbed by appropriate antibiotic therapy; if complicated, drainage to the outside by thoracentesis is necessary.
The distinction between simple and complicated effusion is made by examining a small sample of pleural fluid taken by puncture of the chest wall: if the effusion is simple, it is usually small in volume, contains few white blood cells, has the same glucose concentration as plasma, has a pH > 7.30 and a LDH concentration of 1,000 U/l.
The more these criteria are present, the more immediate the drainage by means of a tube inserted into the pleural cavity must be: if after 48-72 hours the fever persists, it means that the drainage was not complete (due to closed effusions in sealed spaces) or that the antibiotic therapy is wrong or that the diagnosis of infectious pleurisy itself is wrong.
If closed (saccated) effusions are present, surgery is often necessary, with open drainage to prevent the formation of pleuro-bronchial fistulas and spread of the infection to the entire organism (sepsis).
Causes of pleurisy
The factors underlying pleural inflammation are numerous, and we can divide them into the following forms:
- Pleuritis due to infectious agents
They constitute the largest group, due to bacteria, viruses, fungi or parasites.
- Tubercular pleurisies: these represented the most frequent form for many years and even today, despite the considerable decline in tuberculosis, they are far from rare. Pleuritis represents the most frequent form of extra-pulmonary tuberculosis, which mainly affects young patients and can manifest itself with a simple fibrinous inflammation (dry pleuritis) or with abundant exudate production. Contrary to what one might think, the arrival of tuberculous mycobacteria does not occur from the lung, but often from initial extra-pulmonary localisation, with dissemination of Koch’s bacilli through the lymphatic pathways.
- Apart from mycobacteria, brucella (typical pleurisy of cattle breeders and veterinarians), staphylococcus (often in association with pneumonia and with the characteristic formation of purulent ooze), klebsiella, pseudomonas and other less frequent bacteria are often involved in causing pleurisy.
- Viruses can also cause pleurisy, but they are believed to be very rare forms, probably underestimated in frequency due to the diagnostic difficulty of these forms.
- Finally, very rarely, there are pleurisies caused by fungi (aspergilli and candida) and by parasites (entamoeba).
Pleuritis due to immune and/or allergic phenomena
In these forms there is an allergic hypersensitivity of an immediate or delayed type, leading to a more or less marked immune disruption.
They belong to this category:
- Tuberculin hypersensitivity pleuritis, which is not due to aggression by the mycobacterium but to tuberculin stimuli that affect the pleura after the subject has already acquired immunity; they are typical of those who work in environments in contact with tuberculosis patients and they are more prevalent in the young.
- Rheumatic pleuritis, which occurs during acute joint rheumatism, not due to the direct action of streptococcus but to immunological alterations, like all manifestations of rheumatic disease (endocarditis, arthritis, serositis).
- Eosinophilic pleuritis, characterised by a large quantity of eosinophilic leucocytes in the pleural fluid (15%-20% of total leucocytes), not necessarily concomitant with eosinophilia in the blood. They may be caused by an allergic vasculopathy, a parasitosis or be part of a Loeffler syndrome in which the pulmonary infiltrate is not identified.
- Pleuritis by collagenopathies, occurring in connection with rheumatoid arthritis, systemic lupus erythematosus, scleroderma, panarteritis nodosa and dermatomyositis, i.e. in conjunction with collagen disease.
Pleuritis due to metabolic factors
This group includes rare cholesterol pleuritis, usually saccate, often the result of old tubercular serofibrinous effusions.
Dysprotidemias, uremia, histiocytosis X and Gaucher disease can also cause pleuritis. But these are extremely uncommon forms.
Traumatic pleuritis
As the word implies, they are pleuritis related to closed or open trauma of the chest, with immediate (usually haemorrhagic) or late effusion formation, with a serous or fibrinous character.
Some chylous effusions due to traumatic compression of the thoracic duct are also included in this group.
Pleuritis due to cardiovascular factors
Two different types of pleural suffering may occur in the course of cardio-circulatory or cardio-pulmonary diseases: the formation of a transudate, in connection with disturbances of haemodynamics, or the formation of a true exudate, in connection with organic pulmonary processes (pulmonary infarctions) or cardiac processes (cardiac infarction with post-infarct pleurisy, Dressler’s pericarditis).
Tumour-based pleuritis
There are many neoplastic forms involving involvement of the pleura: apart from primary pleural tumours (mesothelioma, asbestosis), we have lung malignancies and pleural metastases of extrapulmonary malignancies (breast cancer, lymphoma).
Symptoms of pleurisy
The entire set of symptoms depends on the type of pleuritis involved.

Dry pleurisy
They often go completely unnoticed, having short-lived and non-specific symptoms, to the point that they are often diagnosed years later, during a chest X-ray examination carried out for other reasons.
If, on the other hand, symptoms are manifest, the main finding is chest pain, which is punctal, fixed, often intense, worsened by coughing, deep inhalations and decubitus on the affected side.
Fever is usually not high, there is impairment of general condition and an insistent dry cough.
On objective examination, there is reduced expansion of the affected hemithorax and marked pain on pressure on the thoracic base.
On percussion there is dullness, while on listening one hears the characteristic pleural rubbing, sometimes very fine (likened to rustling of hair) sometimes rough (likened to the sound of freshly trodden snow).
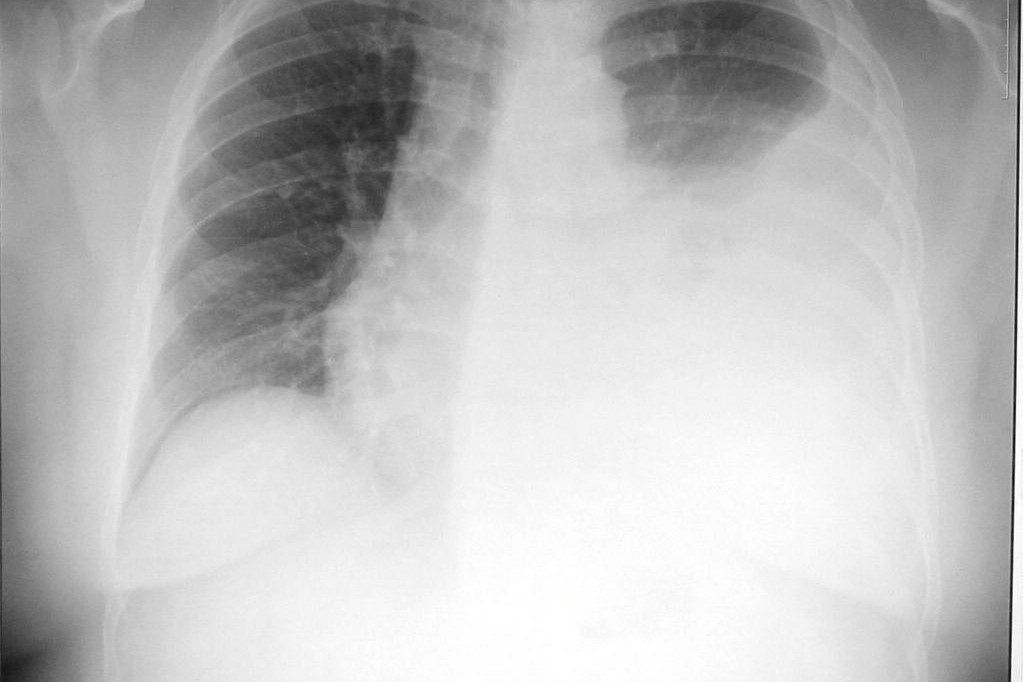
Radiology confirms the diagnosis, with the finding of costo-diaphragmatic sinus veiling.
Exudative pleuritis
They erupt acutely, especially in infectious forms.
The onset is characterised by chills and an abrupt rise in temperature, which quickly reaches 39°-40°, remaining constantly at these levels for 4-5 days and then becoming remittent (the temperature oscillates between two values, both above normal) or intermittent (the temperature oscillates between hyperthermia and normal values).
In rheumatic forms, profuse sweating is common, which, in the case of tubercular infection, occurs especially during the night hours
The most characteristic sign is also in this case chest pain: very early, stinging, burning or gravitating, at a fixed site, worsened by movements, coughing and deep breathing.
As soon as the effusion is established, however, the pain diminishes and sometimes disappears, as does the cough, another frequent symptom.
In parallel with the reduction in coughing and pain, however, an increasing difficulty in breathing is established, due to the fluid occupying the pleural space: tachypnoea (hurried breathing) and dyspnoea (difficulty in breathing) arise, at first on exertion and later also at rest.
At this stage a tachycardia is also constant, from compression on the mediastinum and consequent displacement of the heart
Unlike in dry pleurisy, in exudative pleurisy the patient prefers to lie on the affected side to allow the contralateral lung to expand to its fullest extent: on inspection the affected hemithorax appears increased in volume, often with flattening of the intercostal spaces; on palpation the tactile vocal tremor (the famous ‘say 33’) is diminished or disappeared, and on percussion the hypophonesis is sharp, often reaching true dullness on listening, the vesicular murmur is reduced or abolished, while at the upper limit of the effusion a soft, predominantly expiratory bronchial murmur may be heard, located in the transition zone between the lung crushed by the pleural effusion and the healthy lung above it.
Diagnosis of pleurisy
As always, the clinic must be the fundamental basis of the diagnosis: firstly, the medical history with any exposure of the patient to pathological agents or trauma.
Secondly, the objective examination always carried out according to the classic indications of the old clinical masters: inspection, palpation, percussion and listening, performed in that order, without omitting anything. Finally, the radiological examination that will easily complete and confirm the diagnosis.
Treatment of pleuritis
As always, the therapy must be aetiological, so as to act as soon as possible against the triggering causes, combined with measures to relieve the patient from discomfort: absolute and compulsory bed rest, at least in the initial stages of the disease, with painkillers, anti-inflammatory and antipyretic drugs to partially relieve the symptoms.
In dry pleurisy, mostly of tubercular origin, pharmacological treatment must be directed against the mycobacterium and recourse to antibiotics is mandatory, as in non-tuberculous bacterial forms.
Concomitant to bacterial eradication must be anti-inflammatory and supportive therapy for the patient’s general condition, which may be severely compromised.
In exudative pleurisies, the discourse is similar but even more decisive, since antibiotics and anti-inflammatory drugs must be added to interventions aimed at eliminating the effusion, all the more so if it is imposing: thoracentesis is required in effusions that displace the mediastinum, that cause severe respiratory difficulty or that interfere with the cardiovascular system.
This medical manoeuvre, barring emergencies arising from serious cardio-respiratory situations, should be performed not in the acute phase, but by waiting for a partial resolution of the manifestations, with the patient on the road to recovery.
Direct access into the pleural cavity, moreover, allows drugs (antibiotics and cortisone) to be placed directly at the site of the pleuritic process, with the advantage of an effective antiphlogistic and preventive action on the formation of adhesions that are often the permanent outcomes of pleurisy.
Read Also:
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
Airway Management After A Road Accident: An Overview
Pneumothorax And Haemothorax: Trauma To The Thoracic Cavity And Its Consequences
What Is Empyema? How Do You Deal With A Pleural Effusion?
Pain Management In Blunt Thoracic Trauma
Acute Hyperinflammatory Shock Found In British Children. New Covid-19 Pediatric Illness Symptoms?
What Is Transient Tachypnoea Of The Newborn, Or Neonatal Wet Lung Syndrome?
Traumatic Pneumothorax: Symptoms, Diagnosis And Treatment
Diagnosis Of Tension Pneumothorax In The Field: Suction Or Blowing?
Pneumothorax And Pneumomediastinum: Rescuing The Patient With Pulmonary Barotrauma