
Gallstones: Causes and Symptoms
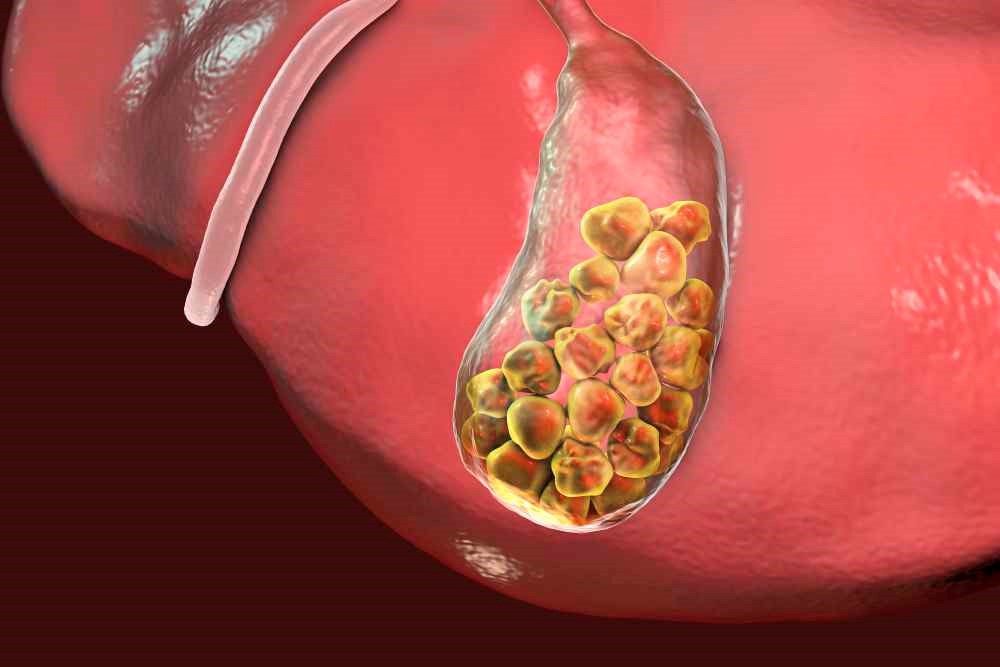
Gallstones appear as small solid stones that form in the gallbladder, also known as the gallbladder, due to a higher concentration of cholesterol in the bile
What is gallstone disease
Gallstone disease is a widespread disease in the Western world, present in percentages ranging from 5% to approximately 25% in the adult population of various American and European countries (especially Northern Europe).
In Europe, the latest data speak of a prevalence of biliary lithiasis that varies from 9 to 19% (about 19% in women and 9.5% in men).
The Italian data, deriving from studies conducted in the 1980s, were able to ascertain that:
- calculi are present in 10% of the general population;
- female subjects are more affected, in double percentages compared to male subjects (15% vs 7%);
- with advancing age the prevalence of the disease increases significantly in both sexes.
What are gallstones
Gallstones are essentially of three types: cholesterol, pigmentary and mixed and can be present in the gallbladder, in the biliary tract or in both of these anatomical structures.
The process of stone formation is slow and has been studied especially in regards to cholesterol stones.
Initially, there is an increased concentration of cholesterol in the bile (due to congenital anomalies of the hepatic metabolism of endogenous fats, due to an incorrect diet or, again, due to a reduction of the bile cholesterol-solubilizing agents), aggregation in nuclei and subsequently into cholesterol crystals, which are then the basis for subsequent calculations.
Practically a bile supersaturated with cholesterol and with a composition of the bile secreted by the hepatocyte in non-ideal proportions of the various types of bile acids necessary and useful for normal digestive function, and perhaps in a context of metabolic syndrome and incorrect diet: this, therefore, it is the pathogenesis for cholesterol stones.
The question relating to pigmented biliary stones, which present a different pathogenesis, is different and more complex.
The gallbladder is the point where stones can most easily form, precisely because there is stagnation of bile inside it when you are fasting and there is time for the nucleation and crystallization of a bile richer in cholesterol.
If the gallbladder presents, due to intrinsic pathologies, a delayed, slow or ineffective emptying, stones are formed more easily.
Pigmented stones represent a minority of gallstones (approximately 20-25% in operative findings) and are so named because of their dark color.
They consist of a mixture of cholesterol, phosphate and calcium carbonate and a particular pigment, bilirubin.
They are generally associated with chronic haematological diseases capable of inducing hemolysis (i.e. destruction of red blood cells) and release of the hemoglobin contained within red blood cells, which is then degraded to form bilirubin.
This type of stone is more common in the elderly and in advanced chronic liver disease.
Causes of gallstones
Obesity is an established risk factor, especially in women: in this condition, genetic or from an incongruous diet, there is an increased synthesis and biliary excretion of cholesterol.
Another risk factor is certainly the infection of the biliary tract, particularly important for the genesis of pigmentary stones.
Age can also be considered a risk factor as the prevalence of stones is markedly increased in the elderly, probably due to the higher concentration of cholesterol in the bile and the hypomobility of the gallbladder.
In the light of these data, considering the progressive increase in the average age of the Italian population, it is conceivable that gallstone disease will become a growing health problem in the coming years.
Pregnancy (especially multiple pregnancies) determines a stagnation of bile in the gallbladder with incomplete emptying and ease of formation of cholesterol crystals, precursors of stones.
Pregnancy associated with obesity further increases the risk.
The use of oral contraceptives is also associated with an increased risk of gallstones.
Finally, the food behaviors most at risk for the development of gallstones are essentially identified in a diet low in fiber and rich in cholesterol and triglycerides.
Gallstones, other contributing factors to be mentioned are also as follows:
- the composition in quantity and quality and the proportion between them of the various components of bile and cholesterol;
- a deficit of gallbladder motility, the sluggish gallbladder, not very mobile, which causes biliary stasis and therefore aggregation of cholesterol crystals;
- a motor defect of the digestive system, such as slowed transit or alteration of peristalsis;
- gallbladder hydrops dangerous for possible various complications, even serious ones (abscess, perforation, etc..)
What are the symptoms of gallstones?
Gallstones can give rise to specific symptoms (such as typical pain, the so-called biliary colic or complications of the disease) or their presence can remain silent (asymptomatic lithiasis).
From these two eventualities arises a completely different decision-making approach.
Biliary colic is defined as pain in the right epigastrium/hypochondrium sometimes radiating posteriorly and to the right shoulder lasting about 30 minutes and not disappearing with defecation.
In addition, there may be nausea and vomiting or dyspepsia (sense of postprandial weight, belching, epigastric swelling, etc.), but the latter are generic symptoms that can also occur in many other situations that do not properly characterize the so-called biliary colic and may be present in lithiasic and non-lithiatic populations.
Important complications, to be brought to the operating table, can be acute lithiasic and non-lithiasic cholecystitis, or bilio-enteric fistulas or stenosis of the ab extrinsic common bile duct due to large cystic duct stones.

Small stones that easily make their way from the bile duct to the sphincter of Oddi can often be responsible for acute pancreatitis and also require cholecystectomy.
Asymptomatic patients may not have any specific symptoms for many years; in them the probability of developing biliary pain is about 10% at 5 years and 20% at 15-20 years, with an annual risk of presenting biliary colic which decreases over time.
In some studies in which it has been possible to monitor patients for a long time, it has been verified that in these patients the annual probability of developing a major complication is about 1%.
On the basis of these data, there is no rationale for an indication for elective prophylactic cholecystectomy in patients with asymptomatic gallstones.
Of course, the matter is completely different in the presence of a symptomatic stone disease, where a therapeutic decision is necessary.
The disease can present with pain, generally due to the passage of stones in the cystic duct or in the common bile duct, or with complications of great clinical importance such as acute cholecystitis with the possibility of infection up to the abscess or perforation of the gallbladder, acute infections of the gallbladder, common bile duct obstruction with jaundice, acute pancreatitis.
These are all clinical occurrences which, if not recognized and treated quickly, can lead to serious, sometimes fatal, complications.
Diagnosis of gallstones
A good anamnestic and clinical investigation already sufficiently leads to the correct diagnosis.
The confirmation comes from laboratory data (increase in so-called bile stasis investigations) and above all from imaging techniques.
Ultrasound is the technique of choice, as it is diagnostic in over 90% of cases, it is non-invasive, relatively inexpensive and reproducible.
In the case of gallstone disease, ultrasound allows you to have other useful information for the general evaluation of the disease and the patient (thickness of the gallbladder, dilatation of the bile ducts, associated hepatic and/or pancreatic pathologies, etc.).
Plain radiography of the abdomen and cholecystography add little to the ultrasound data and are required only in special cases.
Computed tomography (CT) is inferior to ultrasonography in gallstone disease and may be useful in demonstrating the degree of stone calcification in patients in whom stone-dissolving treatment with drugs is attempted.
If the stones are in the biliary tract, the diagnostic problem may not be resolved by ultrasound and other more sophisticated investigations must be resorted to such as nuclear magnetic resonance cholangiography (MRI) or endoscopic retrograde cholangiography, techniques which generally require hospitalization.
Read Also:
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
Kidney Stones: What They Are, How To Treat Them
Creatinine, Detection In Blood And Urine Indicates Kidney Function
How To Keep Your Kidneys Healthy?
Colour Changes In The Urine: When To Consult A Doctor
Paediatric Urinary Calculus: What It Is, How To Treat It
High Leukocytes In The Urine: When To Worry?
The Colour Of Pee: What Does Urine Tell Us About Our Health?
Kidney Function Replacement Treatment: Dialysis
Chronic Kidney Failure: Causes, Symptoms And Treatment
Pancreas: Prevention And Treatment Of Pancreatic Cancer
Gestational Diabetes, What It Is And How To Deal With It
Pancreatic Cancer, A New Pharmacological Approach To Reduce Its Progression
What Is Pancreatitis And What Are The Symptoms?
Kidney Stones: What They Are, How To Treat Them
Acute Pancreatitis: Causes, Symptoms, Diagnosis And Treatment
Kidney Cancer: Laparoscopic Surgery And The Latest Technologies