
Valvulopathies: examining heart valve problems
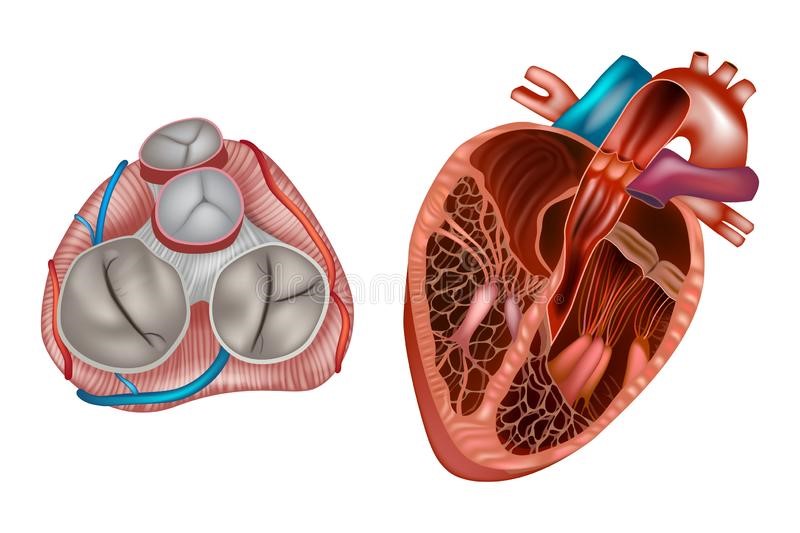
Let’s talk about valvulopathies: heart valves are the structures that separate the cardiac chambers (atria and ventricles) from each other and from the great vessels (aorta and pulmonary artery)
There are four heart valves (tricuspid, pulmonary, mitral and aorta), which are able to open and close in coordination with the heartbeat, so that blood can only pass in one direction.
Diseases of the heart valves are called valvulopathies and can be of two types: stenosis (incomplete opening; blood passes through a smaller than normal orifice) and insufficiency (incomplete closure; part of the blood flows back through the valve that should be closed).
Very often, however, stenosis and insufficiency coexist, to varying degrees, in the same valve, resulting in what is known as stenoinsufficiency.
Valvulopathies can be congenital, i.e. present from birth, or acquired (appearing in the course of life)
The latter can be of degenerative origin (more frequent in elderly, often hypertensive subjects, essentially due to wear and tear of the valve structures), infectious (endocarditis), ischaemic (during an acute myocardial infarction), traumatic (very rarely) or secondary to conspicuous dilatation of the ventricle and/or great vessels.
The course of valvulopathies is in most cases slowly progressive, with an even very long phase (years) of complete asymptomaticity.
If, however, valvulopathy arises acutely on a hitherto normal valve (following trauma, myocardial infarction, endocarditis with perforation of the valve leaflets), the clinical presentation can be dramatic.
Diseases of the valves of the right sector of the heart (tricuspid and pulmonary), where a lower pressure regime applies, are rare and usually due to congenital problems.
Mitral and aorta diseases, on the other hand, are much more frequent.
Causes of valvulopathies
Congenital valvulopathies are due to alterations in the embryonic development of cardiac structures and are often associated with other congenital anomalies that result in very complex syndromes.
Acquired valvulopathies may be due to infection, inflammation, degeneration of valve tissue, trauma, myocardial ischaemia or pathologies of the heart muscle or ascending aorta.
In past decades, one of the main causes of valvulopathy was rheumatic valve disease, which arises as a complication of pharyngitis or tonsillitis caused by a particular bacterium.
The heart valves are affected a few weeks after the tonsillar infection.
They become damaged and progressively deformed.
Nowadays, with improved living conditions, fewer infections and longer life spans, the most frequent cause of valvulopathy is degenerative, i.e. due to the progressive damage to the valve structure that occurs with age.
Consequences of valve disease
The consequences of valve disease depend on the type of abnormality (stenosis or insufficiency) and its severity.
The extreme consequence of any valvulopathy is heart failure.
Although it is difficult to generalise, it can be said that every valvulopathy goes through two phases: a first one of compensation, during which the heart puts in place a series of mechanisms to cope with the problem, and a second one that evolves towards heart failure, when the adaptation mechanisms are no longer sufficient to maintain an adequate cardiac output.
Valvular stenosis causes an increase in pressure upstream of the diseased valve.
In the case of aortic or pulmonary valve involvement, the ventricles undergo hypertrophy (increased wall thickness), which enables them to generate a higher pressure for a certain period of time, while in the case of mitral or tricuspid valve involvement, the atria, whose wall thickness is very small, undergo dilatation.
Dilation of the atrial chambers often causes the onset of atrial fibrillation, an arrhythmia that further worsens cardiac function.
At a certain point, the ventricles are no longer able to further increase their thickness and they too begin to dilate excessively.
The evolution at this point is towards heart failure
In valve failure, on the other hand, the affected heart chambers receive an excessive amount of blood due to regurgitation through the valve, which closes imperfectly.
Since they do not have to overcome increased resistance, they do not need to increase their wall thickness and react to the volume overload by dilating.
When the dilatation is too marked, the heart can no longer contract properly and blood pooling occurs in the pulmonary vascular bed (pulmonary oedema), in the liver (hepatomegaly, abdominal swelling) and in the lower limbs (oedema or swelling).

Valvulopathies: symptoms
The patient with valvulopathy is often asymptomatic or not very symptomatic even up to an advanced stage.
For this reason, the main risk is that diagnosis and treatment come too late.
Once the heart is excessively dilated, in fact, even if the diseased valve is replaced, there is no improvement in the clinical condition and the patient goes into progressive heart failure.
The symptoms depend on the type of valvulopathy.
The first symptoms are usually the appearance of easy fatigability, dyspnoea (difficulty breathing) during physical activity and later at rest.
Patients may experience heart palpitations due to the onset of arrhythmias such as atrial fibrillation.
Sometimes the first clinical sign may be a stroke, due to parts of clots forming within the dilated heart chambers entering the bloodstream.
If the right ventricle is involved, liver congestion and declivous oedema (fluid retention in the lower limbs) appear.
In the presence of aortic stenosis, the patient may experience angina, syncope (fainting) or even sudden death.
In order to experience fewer problems, the patient often unconsciously decreases his or her physical activity.
For this reason, the degree of functional limitation is often underestimated.
Read Also:
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
What Is The Difference Between Pacemaker And Subcutaneous Defibrillator?
Heart Disease: What Is Cardiomyopathy?
Inflammations Of The Heart: Myocarditis, Infective Endocarditis And Pericarditis
Heart Murmurs: What It Is And When To Be Concerned
Broken Heart Syndrome Is On The Rise: We Know Takotsubo Cardiomyopathy
Cardiomyopathies: What They Are And What Are The Treatments
Alcoholic And Arrhythmogenic Right Ventricular Cardiomyopathy
Difference Between Spontaneous, Electrical And Pharmacological Cardioversion
What Is Takotsubo Cardiomyopathy (Broken Heart Syndrome)?
Dilated Cardiomyopathy: What It Is, What Causes It And How It Is Treated
Heart Pacemaker: How Does It Work?
World Heart Day 2022: Moves For A Healthy Heart
Heart Disease Facts And Statistics: What You Need To Know
What Is Cardiac Transplantation? An Overview