
What is a Cardioverter? Implantable defibrillator overview
Cardioverter – what do we mean by implantable defibrillator? The need for arrhythmia treatment depends on the symptoms and severity of the arrhythmia
Treatment is aimed at the causes.
If necessary, direct anti-arrhythmic therapy is used, which includes anti-arrhythmic drugs, cardioversion-defibrillation, implantable cardioversion-defibrillation, pacemakers (and a special form of electrical stimulation, cardiac resynchronisation therapy), catheter ablation, surgery or a combination of these.
The implantable cardioverter-defibrillator cardioverts or defibrillates the heart in response to ventricular tachycardia or ventricular fibrillation
The most modern implantable cardioverter-defibrillators also have an antibradycardiac and antitachycardiac pacing function (to interrupt atrial or ventricular tachycardias) and are capable of recording intracardiac electrograms.
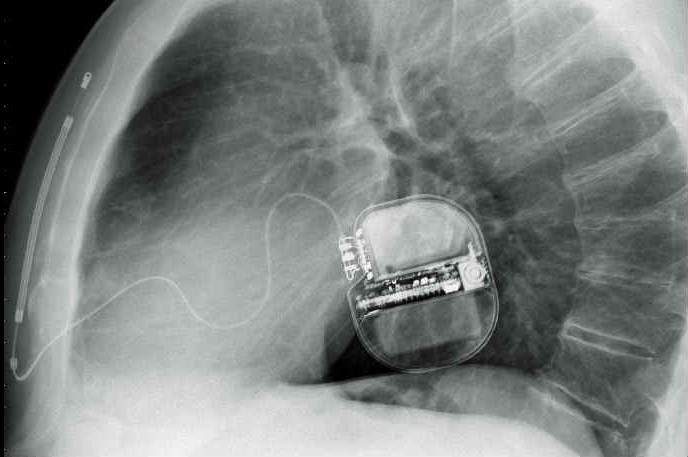
Implantable cardioverter-defibrillators are implanted subcutaneously or subpectorally, with leads inserted transvenously into the right ventricle and sometimes into the right atrium.
A biventricular cardioverter defibrillator also has a left ventricular epicardial electrode placed via the coronary venous sinus or by thoracotomy to allow cardiac resynchronisation therapy.
Implantable cardiac defibrillator types also include a fully implantable cardiac defibrillator implanted subcutaneously without intravascular components and a vest-like wearable defibrillator for short-term use.
The battery life of implantable cardioverter-defibrillator generators is usually about 5 to 7 years.
Indications for implantable defibrillators/cardioverters
Implantable defibrillators/cardioverters are the treatment of choice for patients who have had
- A haemodynamically significant episode of ventricular fibrillation or ventricular tachycardia, not due to reversible or transient conditions (e.g. dysionias, proarrhythmic effect of antiarrhythmic drugs, acute myocardial infarction)
Implantable cardioverter-defibrillators are also indicated in patients with inducible ventricular tachycardia or ventricular fibrillation during electrophysiological study and in patients with idiopathic or ischaemic cardiomyopathy, left ventricular ejection fraction < 35% and high risk of ventricular tachycardia or ventricular fibrillation.
Since implantable cardioverter-defibrillators aim more to treat than to prevent ventricular tachycardia or ventricular fibrillation, patients predisposed to these arrhythmias may require, in addition to the implantable defibrillator, anti-arrhythmic drugs to reduce the number of episodes and thus the need for annoying shocks; this approach also increases the duration of the implantable defibrillator.
Cardioverter – implantable defibrillator malfunctioning
Implantable defibrillators/cardioverters can malfunction

- By delivering inappropriate pacing or discharges
- By not delivering pacing or shocks when needed
Inappropriate pacing or shocks from the implantable cardioverter-defibrillator may occur in response to a sinus rhythm, atrial fibrillation, atrial flutter, or non-physiological impulses (e.g., electrode breakage).
Implantable cardioverter-defibrillators may not be appropriate for appropriate pacing or shock when needed due to factors such as generator or electrode migration, stimulator insensitivity, increased pacing or defibrillation threshold due to endocardial fibrosis at the site of previous shocks, and battery depletion.
When an implantable cardioverter-defibrillator discharges
In patients who report that the implantable cardioverter-defibrillator has discharged but without associated symptoms of syncope, dyspnoea, chest pain or persistent palpitations, follow-up with clinical and/or electrophysiologist implantable cardioverter-defibrillator within one week is indicated.
The implantable cardioverter-defibrillator can then be questioned to determine the reason for the shock.
If, on the other hand, the above symptoms were associated, or the patient received more than one shock, the patient should be sent to the emergency department to search for a treatable cause (e.g. myocardial ischaemia, electrolyte disturbance) or a device malfunction.
Read Also:
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
‘D’ For Deads, ‘C’ For Cardioversion! – Defibrillation And Fibrillation In Paediatric Patients
Inflammations Of The Heart: What Are The Causes Of Pericarditis?
Do You Have Episodes Of Sudden Tachycardia? You May Suffer From Wolff-Parkinson-White Syndrome (WPW)
Knowing Thrombosis To Intervene On The Blood Clot
Patient Procedures: What Is External Electrical Cardioversion?
Increasing The Workforce Of EMS, Training Laypeople In Using AED
Difference Between Spontaneous, Electrical And Pharmacological Cardioversion