
What is anorexia nervosa? Symptoms and treatment of this nutrition disorder
Anorexia nervosa was included in the DSM 5 (2013) in the broader diagnostic category called Nutrition and eating disorders
The main characteristic of this disorder is the rejection of food.
The term anorexia (literally lack of appetite) is not correct to describe a disorder in which the appetite is in most cases preserved.
Rather, what characterises the anorexic person is the terror of gaining weight and the need to control eating in pursuit of thinness.
In individuals with symptoms of anorexia nervosa, self-esteem levels are strongly influenced by physical fitness and body weight.
Weight loss is regarded as an extraordinary achievement and a sign of strict self-discipline, while weight gain is experienced as an unacceptable loss of control.
Anorexia nervosa, the symptoms
A person is anorexic if they manifest the following characteristics:
- Restriction of calorie intake in relation to needs. This leads to a significantly low body weight in relation to age, development and physical health.
- Intense fear of gaining weight or becoming fat.
- Excessive influence of weight or body shape on self-esteem levels.
Two types of anorexia nervosa are also identified:
- Restricted type: in the last three months the person has not presented episodes of binge eating or elimination behaviour. That is, weight loss is mainly achieved through dieting, fasting and/or excessive physical activity.
- Type with binge/elimination behaviour: in the last three months, the person has presented recurrent episodes of binge eating or elimination behaviour (e.g. self-induced vomiting, use of laxatives, diuretics…).
Compared to the previous diagnostic classification, the criterion of amenorrhoea has been eliminated in DSM 5. This is no longer necessary to formulate the diagnosis of anorexia.
In order to avoid gaining weight, those who suffer from the symptoms of anorexia engage in a series of behaviours typical of the disorder.
For example:
- following a strict diet
- exercising excessively
- inducing vomiting after eating even small amounts of food
Incidence and causes of anorexia nervosa
The incidence of anorexia nervosa appears to be stable since 1970 at around 5-5.4 cases per 100,000 inhabitants per year.
The peak incidence is between the ages of 15 and 19. Around this age, adolescents are confronted with sexuality and changes in their bodies.
It rarely occurs in the prepubertal period, although in such situations the clinical picture would be more severe.
The disorder rarely occurs in women over 40.
The prevalence of anorexia seems to be far greater in industrialised countries, where there is an abundance of food and where the value of thinness is emphasised.
This eating disorder manifests itself predominantly in the female sex.
The entry into anorexia nervosa is almost always through the start of a diet.
In any case, from a deliberate attempt to lose weight in order to achieve the ideal of feminine beauty so much vaunted by modern society.
The causes of the eating disorder are not known, but individual risk factors can be identified:
- Conditions present in family members (e.g. the presence of an eating disorder in one of the parents or obsessive and perfectionistic personality traits).
- Experiences prior to the onset of psychopathology (relationship problems with parents, sexual abuse, experiences of mockery because of weight or body shape).
- Individual characteristics such as low self-esteem, perfectionism, anxiety disorders, etc.
Course of the anorexic disorder
The evolution and outcomes of anorexia nervosa are extremely variable.
In some cases, an episode of anorexia is followed by complete remission.
In others, phases of remission, with recovery of body weight, alternate with phases of flare-ups.
Still others present a chronic evolution, with progressive deterioration over the years.
Hospitalisation may be necessary to restore body weight or correct electrolyte imbalances.
Long-term mortality from anorexia nervosa is greater than 10% among those admitted to hospital.
Death usually occurs in connection with malnutrition, electrolyte imbalances, and suicide.
Maintenance factors of anorexia nervosa
The main specific maintenance factor is the over-assessment of weight, body shape and their control.
These are used as the main system for evaluating oneself and one’s worth.
The iron diet is both a symptom and a powerful maintenance factor for the psychopathological core.
An iron diet produces another symptom, low weight, which in turn, causes malnutrition syndrome.
In addition to causing physical damage, low weight contributes to triggering worries about nutrition, food and the body,
This, in fact, maintains the eating problem.
Frequently, in addition to the strict diet, there is also excessive and compulsive exercise.
This maintains concerns about one’s body shape and weight control.
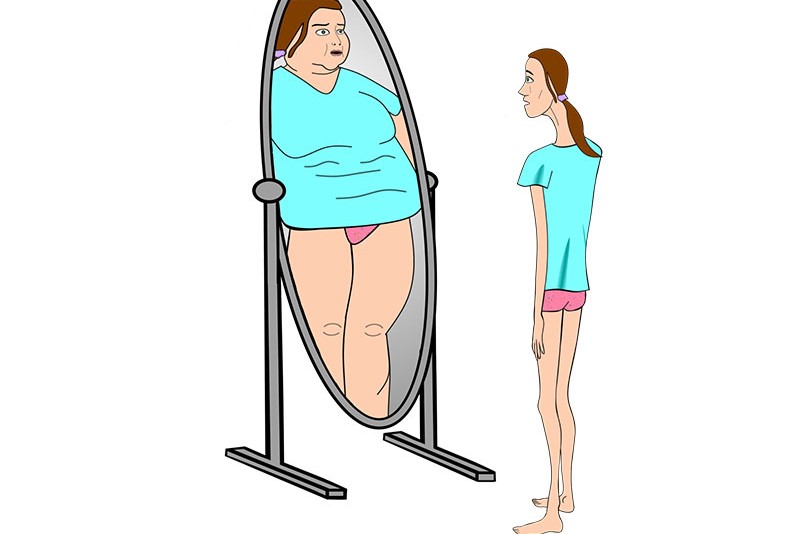
People suffering from anorexia nervosa place an excessive value on physical appearance and body weight.
Some feel fat in reference to the totality of their body.
Others, while admitting their thinness, perceive certain body parts as ‘too fat’.
These are usually the abdomen, buttocks and thighs.
They may adopt the most diverse techniques to assess body size and weight.
For example, constantly weighing themselves, obsessively measuring themselves with a tape measure, or checking perceived ‘fat’ parts in the mirror.
Frequent body checks act as maintenance factors.
In fact, they increase concern over the slightest perceived or recorded changes and encourage strict dieting.
Effects of malnutrition

Although some anorexics may realise their thinness, they typically deny the serious physical health consequences of their condition.
Many signs and symptoms of anorexia are related to extreme malnutrition.
In addition to the absence of menstruation (amenorrhoea), they may complain of
- constipation
- abdominal pain
- intolerance to cold
- lethargy or excess energy
- marked hypotension
- hypothermia
- dryness of the skin
- lanugo (a fine, soft down) on the trunk
- bradycardia
In those who engage in the practice of self-induced vomiting, erosions of the dental enamel can also be found. In addition, scars or calluses are found on the back of the hands.
These are caused by rubbing against the dental arch in an attempt to induce vomiting.
A state of malnutrition also causes emotional and social changes such as:
- Depression
- Anxiety
- Irritability and anger
- Mood swings
- Social isolation
Cognitive changes such as:
- Decreased capacity for abstract thought
- Decreased ability to concentrate
Anorexia nervosa, treatment
The treatment of anorexia should ideally be conducted on an outpatient basis.
However, this is not always possible and is only indicated for patients with certain characteristics:
- BMI not less than 15
- absence of medical complications
- real motivation to change
- presence of a favourable family environment
Otherwise, specialised hospital intervention may be appropriate.
Psychotherapy for anorexia nervosa
All proven effective treatments for anorexia nervosa are psychological in nature.
At present, research shows that cognitive behavioural therapy CBT-E is the best treatment choice for eating disorders.
CBT-E (enhanced cognitive behavioural therapy) was developed at Oxford University by Christopher Fairburn.
It is a specific form of cognitive behavioural therapy focused on the psychopathology of eating disorders.
CBT-E aims to address the specific psychopathology of the eating disorder and the processes that maintain it.
It adopts specific strategies and tools aimed at modifying problematic behaviour and reducing the absolute need for thinness.
The treatment of anorexia nervosa involves 3 steps:
- The objective of the first step is to help people come to the conclusion to deal with their eating problem. That is, to prepare them for an active change.
- Step two, on the other hand, has two objectives: to help the person with anorexia reach a low healthy weight (BMI between 19 and 20) and to address the psychopathology (e.g. body image form). Also within step 2, work is done on recognising problematic mental states in order to avoid backward steps. The duration of this step depends on the amount of weight to be recovered.
- The last step aims to address concerns about the end of treatment and to prevent relapse risks.
Pharmacological therapy of anorexia
Pharmacological studies are scarce and do not demonstrate a beneficial effect of drugs on the disorder.
The most reasonable approach is not to use any drugs in the acute phase of weight loss.
This is because depressive and obsessive-compulsive symptoms often decrease with weight gain.
If, however, depression persists after reaching an adequate body weight, antidepressants may be useful.
Occasionally, anxiolytics, benzodiazepines, taken before meals, may be used: however, their usefulness seems limited.
The use of antipsychotics is reserved only for the most difficult and refractory patients.
Bibliographical references
- In Fairburn, C.G. (2008). Cognitive Behavior Therapy and Eating Disorders. New York: Guilford Press. (trad. it. La terapia cognitivo comportamentale dei disturbi dell’alimentazione, Trento: Centro Studi Erickson, 2018).
- Dalle Grave, R. (2013). Multistep cognitive behavioral therapy for eating disorders: Theory, practice and clinical cases. New York: Jason Aronson (trad. it. La terapia cognitivo comportamentale multistep per i disturbi dell’alimentazione, Trento: Centro Studi Erickson, 2019).
- Dalle Grave, R. (2016). Come vincere i disturbi dell’alimentazione: Un programma basato sulla terapia cognitivo comportamentale. Verona: Positive Press.
Read Also
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
Bulimia: How To Recognize It And How To Cure It
BMI: How To Calculate Body Mass Index
Mindful Eating: The Importance Of A Conscious Diet
How To Deal With Eating Disorders
Eating Disorders In Children: Is It The Family’s Fault?
Eating Disorders: The Correlation Between Stress And Obesity
Obstructive Sleep Apnoea: What It Is And How To Treat It
Obesity In Middle Age May Influence Earlier Alzheimer’s Disease
Anorexia Nervosa: The Risks For Adolescents
Paediatrics / ARFID: Food Selectivity Or Avoidance In Children
Gaslighting: What Is It And How To Recognise It?
Eco-Anxiety: The Effects Of Climate Change On Mental Health
Separation Anxiety: Symptoms And Treatment
Generalised Anxiety Disorder And Panic Attacks: Diagnosis And Treatment