

Long QT syndrome: causes, diagnosis, values, treatment, medication
Long QT syndrome (LQTS) refers to a set of symptoms caused by a cardiac abnormality characterised by delayed repolarisation of myocardial cells and associated with syncope (fainting with loss of consciousness and postural tone)
Syncope is most often caused by malignant arrhythmias, especially tip torsions, which can degenerate into ventricular fibrillation, leading to irreversible cardiac arrest of the affected person (sudden cardiac death).
Arrhythmias in LQTS patients are often triggered by exercise or very strong emotional stimuli, such as terror.
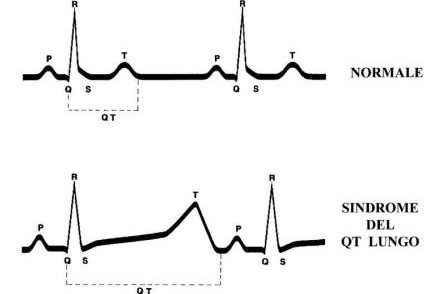
Individuals with LQTS have a characteristic prolongation of the QT interval on the electrocardiogram: this interval is measured from the beginning of the Q wave to the end of the T wave (see image above).
Underlying all forms of LQTS is an abnormal repolarisation of the myocardium.
Abnormalities in repolarisation cause differences in myocardial refractoriness.
Because of these differences, any afterdepolarisations (which occur more frequently in LQTS patients) can propagate to adjacent cells, leading to re-entry ventricular arrhythmias.
Epidemiology and risk factors in Long QT syndrome (LQTS)
In genetically predisposed individuals, sudden increases in sympathetic tone, such as can occur during excessive exertion or violent emotions, are risk factors for the onset of malignant arrhythmias.
The syndrome predominantly affects young women. Among those affected, the incidence of tip torsion, syncope and sudden cardiac death is higher in the case of congenital deafness, previous tachyarrhythmia or syncope; it also increases in proportion to the lengthening of the QT interval.
The relative risk of malignant arrhythmias is estimated to increase 1.1 – 1.2-fold for each 10 msec prolongation of the QTc interval beyond normal values.
Clinical variants
We distinguish two different congenital syndromes characterised by prolongation of the QT interval and risk of sudden death due to ventricular arrhythmias:
- Romano-Ward syndrome, which is inherited according to the autosomal dominant model (not associated with congenital neurological deafness or other congenital heart diseases, autism, complete syndactyly and immunodeficiency).
- Jervell-Lange-Nielsen syndrome, which is inherited in the autosomal recessive pattern (associated with congenital neurological deafness or other congenital heart diseases, autism, complete syndactyly and immunodeficiency).
Causes of LQTS
There are two forms of LQTS: congenital (rarer) and acquired (more frequent).
Acquired forms
Most cases seen in clinical practice involve acquired forms, which can be divided into two categories: those generated by disorders of the hydro-electrolyte balance and those dependent on drug administration.
Forms induced by electrolyte disorders
- hypokalaemia
- hypomagnesaemia
- hypocalcaemia
- Drug-induced forms
- antiarrhythmic drugs
- Quinidine
- Amiodarone
- Sotalol
- Procainamide
- Ranolazine
- Anti-histamines
- terfenadine
- astemizole
- mizolastine
- Macrolide antibiotics
- Erythromycin
- Certain fluoroquinolone antibiotics
- Major anxiolytics
- Tricyclic antidepressants
- Agents active on gastro-intestinal motility
- Cisapride
- Domperidone
- Antipsychotic drugs
- Haloperidol
- Quetiapine
- Thioridazine
- Droperidol
- Analgesics
- Methadone
- LAAM
Just like congenital forms of LQTS, acquired forms can lead to life-threatening arrhythmias.
Treatment consists of correcting the electrolyte imbalance, resolving its cause, and discontinuing therapy with the drug indicative of QT prolongation.
Given its wide use, tendency for interactions with other drugs, and inherent ability to cause QT interval prolongation, erythromycin is probably the predominant cause of acquired long QT syndrome.
In fact, erythromycin use is associated with an incidence of sudden death more than double that of other antibiotics.
In addition to the two major categories listed above, it must be remembered that there are other causes of QT interval prolongation such as anorexia nervosa, hypothyroidism, HIV infection, myocarditis and myocardial infarction.
Congenital forms
Congenital forms of LQTS can be determined by mutations in one of several genes identified to date.
These mutations tend to prolong the duration of the ventricular action potential (APD), thus lengthening the QT interval.
The congenital forms can be inherited as an autosomal dominant or autosomal recessive character.
The autosomal recessive form is associated with other congenital heart diseases, autism, complete syndactyly and immunodeficiency (LQTS8) or with congenital neurological deafness (LQTS1).
An increasing number of gene loci are being identified in association with LQTS. Genetic testing for LQTS is available in clinical practice and can also help in setting the appropriate therapy (Overview of LQTS Genetic Testing).
The most common causes of LQTS involve mutations in the KCNQ1 (LQTS1), KCNH2 (LQTS2) and SCN5A (LQT3) genes.
Jervell and Lange-Nielsen syndrome
It is the autosomal recessive form of LQTS.
It is associated with congenital neurological deafness or other congenital heart diseases, autism, complete syndactyly and immunodeficiency.
It is specifically caused by a mutation in the KCNE1 and KCNQ1 genes.
Of untreated individuals, approximately 50% die by the age of 15 years due to ventricular arrhythmias.
Romano-Ward syndrome
Romano-Ward syndrome is the autosomal dominant form of LQTS.
It is not associated with congenital neurological deafness or other congenital heart diseases, autism, complete syndactyly and immunodeficiency.
Diagnosis and values of Long QT Syndrome:
The diagnosis of LQTS is often not easy since 2.5% of the healthy population has a prolonged QT, and 10-15% of LQTS patients have a normal QT interval: often even some professional athletes may have it without medical personnel noticing.
A commonly used diagnostic criterion is based on the LQTS ‘diagnostic score’.

The score is calculated by assigning points according to various criteria listed below.
With 4 or more points the probability of LQTS is high, and with 1 point or less the probability is low; 2 or 3 points indicate an intermediate probability.
QTc (defined as QT interval/square root of RR interval)
- >= 480 msec – 3 points
- 460-470 msec – 2 points
- 450 msec and male gender – 1 point
- Ventricular torsades de pointes type tachycardias – 2 points
- T wave alternation – 1 point
- T wave avalanche in at least 3 leads on ECG – 1 point
- Low heart rate for age (children) – 0.5 points
- Syncope (no points can be awarded for both syncope and peak torsion in the same subject)
- Under stress conditions – 2 points
- Outside of stress conditions – 1 point
- Congenital deafness – 0.5 points
- Family history (the same family member cannot be counted for both sudden death and LQTS)
- Other family members with definite diagnosis of LQTS – 1 point
- Sudden death in close family members (members under 30 years of age) – 0.5 points
Therapy
In asymptomatic patients without demonstration of ventricular arrhythmias and in the absence of a positive family history of sudden death, observation alone and possibly drug therapy without the need to go to the maximum tolerated dosage is recommended.
In LQTS1 and LQTS2, beta-blockers may be used; in LQTS 3, class Ib anti-arrhythmics such as mexiletine are preferable.
The same drugs can be used to treat emergency patients, with the caveat that only lidocaine should be used until the diagnosis of LQTS1 or LQTS2 is confirmed, as beta-blockers may worsen arrhythmias in LQTS3 patients.
Anti-arrhythmic therapy should, however, be adopted and conducted at the maximum tolerated dosage in those patients who are asymptomatic but have evidence of non-sustained ventricular arrhythmias and a family history of sudden death.
Implantable cardioverter defibrillator (ICD) implantation is not strictly recommended in these patients.
The latter is, however, absolutely indicated (class I indication) in patients with syncope or who have already had an episode of cardiac arrest.
The device’s pace-maker function must be exploited in those who present arrhythmias during bradycardia or pauses in heart rhythm.
In patients who still present symptoms despite optimal medical therapy, left cervical-thoracic gangliectomy surgery is indicated, with destruction of the stellate ganglion and the first three or four thoracic sympathetic ganglia.
Prognosis and risk
For untreated LQTS patients, the risk of an event (syncope or cardiac arrest) can be estimated by knowing their genotype (LQTS1-10), gender and QTc interval.
High risk (>50%)
QTc>500 msec LQTS1 & LQTS2 & LQTS3 (males)
Intermediate risk (30-50%)
QTc>500 msec LQTS3 (females)
QTc<500 msec LQTS2 (females)& LQTS3
Low risk (<30%)
QTc<500 msec LQT1 & LQT2 (males)
Long QT syndrome and sport
Patients with LQTS, under strict cardiological control, can still play sports, but avoid those that include prolonged high exertion and water sports such as swimming and diving.
Read Also:
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
Heart Disease: What Is Cardiomyopathy?
Inflammations Of The Heart: Myocarditis, Infective Endocarditis And Pericarditis
Heart Murmurs: What It Is And When To Be Concerned
Broken Heart Syndrome Is On The Rise: We Know Takotsubo Cardiomyopathy
What Is A Cardioverter? Implantable Defibrillator Overview
‘D’ For Deads, ‘C’ For Cardioversion! – Defibrillation And Fibrillation In Paediatric Patients
Inflammations Of The Heart: What Are The Causes Of Pericarditis?
Do You Have Episodes Of Sudden Tachycardia? You May Suffer From Wolff-Parkinson-White Syndrome (WPW)
Knowing Thrombosis To Intervene On The Blood Clot
Patient Procedures: What Is External Electrical Cardioversion?
Increasing The Workforce Of EMS, Training Laypeople In Using AED
Difference Between Spontaneous, Electrical And Pharmacological Cardioversion
What Is Takotsubo Cardiomyopathy (Broken Heart Syndrome)?
The Patient’s ECG: How To Read An Electrocardiogram In A Simple Way
Stress Exercise Test Inducing Ventricular Arrhythmias In LQT Interval Individuals