
Percutaneous Transluminal Coronary Angioplasty (PTCA): What is it?
Percutaneous Transluminal Coronary Angioplasty (PTCA) is an interventional cardiology technique first performed in 1977 by a German physician, Dr Andreas Gruentzing
It is estimated that between 500,000 and 600,000 angioplasties are currently performed worldwide each year and that in the United States, with 300,000 procedures per year since 1990, angioplasty has surpassed bypass surgery.
In Italy, the method’s expansion has seen slower growth due to organisational reasons: in order to cope with possible acute complications linked to the procedure, angioplasty must necessarily be performed in the presence of a cardiac surgery standby, with a cardiac surgery operating theatre ready when needed for the immediate performance of an emergency restorative operation; obviously, this limits the operational possibilities of the various centres.
What percutaneous transluminal coronary angioplasty consists of
The first step in performing percutaneous transluminal coronary angioplasty is the visualisation of the coronary arteries by means of coronarography.
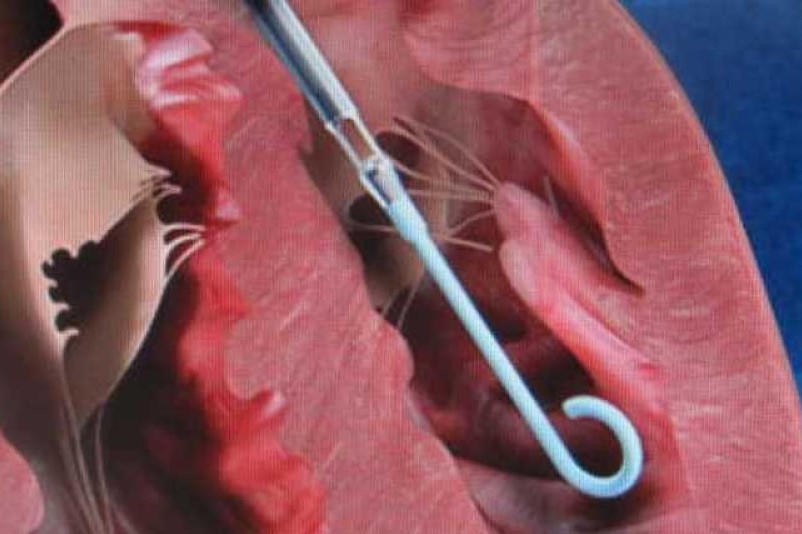
Once the stenotic section of the coronary vessel is highlighted, a catheter equipped at its end with a small inflatable balloon is advanced to that point.
Inflating the balloon at a pressure of several atmospheres induces a barotrauma, which crushes the atherosclerotic plaque obstructing its lumen along the vessel walls, thus eliminating the stenosis of the vessel and restoring good flow downstream.
This is a very elegant and sophisticated technique that requires great skill on the part of the operators and is the result of a very high level of bioengineering technology in the design and construction of the catheters, which are high-precision, highly sophisticated and very expensive instruments.
Initially, angioplasty was performed in selected cases that gave the greatest guarantee of success: on a single vessel, when this was easily reached by the catheter, and in the presence of stenosis that was not long and not tight.
Later, as the technique was perfected and the materials improved, the method was also increasingly used in complex situations, e.g. on several vessels at the same time.
Whenever possible, angioplasty is also usefully employed in the treatment of venous bypass occlusion.
How to prepare for percutaneous transluminal coronary angioplasty
The procedure is performed in the haemodynamic room, does not require narcosis, and involves a hospital stay of only 24-48 hours.
In general, immediate dilatation success rates are very high, with more than 90% of cases treated overall; however, angioplasty presents a major problem, which is still unresolved: in between 30% and 40% of cases, the result obtained initially disappears over time, so that the dilatation obtained is cancelled and the stenosis reappears.
The highest incidence of restenosis generally occurs quite early, within the first six months after dilatation.
In addition to pharmacological treatments, which have on the whole proved to be poorly effective, other interventional avenues have been attempted to avoid or limit the incidence of restenosis.
The best results, in this respect, have been obtained with the use of prosthetic implants such as stents, which are small cages or very elastic, metal fenestrated tubes that, again guided by the catheter, are introduced into the vessel until they reach the stenosis and positioned, dilated and left in place.
The use of stents has led to a reduction in the incidence of restenosis at a rate of less than 20%; moreover, stents have proved very effective both in obtaining more satisfactory and stable results after balloon dilatation and, above all, in obviating acute occlusion of the vessel immediately after angioplasty, a very risky and dreaded complication.
Irrespective of the possible use of stents, in the event of restenosis it is generally also possible to repeat the dilation procedure
The risks in the case of percutaneous transluminal coronary angioplasty are, on the whole, quite low and acceptable: the risk of procedure-related death is recently estimated to be around 0.3%, the risk of infarction around 0.9%, and the risk of having to resort to emergency bypass surgery around 1.8%.
The choice, in the individual patient, must be made on the basis of an exact prediction of the best results and expected benefits with each of the treatment options.
On the other side of the scales are the difficulties and risks specific to each of the therapeutic choices, such as: ineffectiveness of medical therapy or impossibility of performing it because of serious intolerance; prohibitive conditions for bypass due to very old age or serious concomitant pathologies; high risk associated with angioplasty or foreseeable serious difficulties in its performance.
Nowadays, economic evaluations cannot be disregarded either: bypass is certainly more expensive than angioplasty, however, the possible need to repeat the dilation procedure or the use of stents can lead to costs that are very close to being equal.
Read Also:
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
Carotid Angioplasty And Stenting: What Are We Talking About?
Atrial Fibrillation: Symptoms To Watch Out For
Coronary Angioplasty, What To Do Post-Operatively?
Heart Patients And Heat: Cardiologist’s Advice For A Safe Summer
US EMS Rescuers To Be Assisted By Paediatricians Through Virtual Reality (VR)

Coronary Angioplasty, How Is The Procedure Performed?
Atrial Fibrillation: Causes, Symptoms And Treatment
Cardiac Rhythm Disturbance Emergencies: The Experience Of US Rescuers
Prenatal Pathologies, Congenital Heart Defects: Pulmonary Atresia
Management Of Cardiac Arrest Emergencies
Palpitations: What Causes Them And What To Do
The J-Curve Theory In High Blood Pressure: A Really Dangerous Curve
Why Children Should Learn CPR: Cardiopulmonary Resuscitation At School Age
What Is The Difference Between Adult And Infant CPR
Long QT Syndrome: Causes, Diagnosis, Values, Treatment, Medication
What Is Takotsubo Cardiomyopathy (Broken Heart Syndrome)?
The Patient’s ECG: How To Read An Electrocardiogram In A Simple Way
Stress Exercise Test Inducing Ventricular Arrhythmias In LQT Interval Individuals
CPR And Neonatology: Cardiopulmonary Resuscitation In The Newborn
First Aid: How To Treat A Choking Baby
How Healthcare Providers Define Whether You’re Really Unconscious
Concussion: What It Is, What To Do, Consequences, Recovery Time
AMBU: The Impact Of Mechanical Ventilation On The Effectiveness Of CPR
Defibrillator: What It Is, How It Works, Price, Voltage, Manual And External
The Patient’s ECG: How To Read An Electrocardiogram In A Simple Way
Emergency, The ZOLL Tour Kicks Off. First Stop, Intervol: Volunteer Gabriele Tells Us About It
Proper Defibrillator Maintenance To Ensure Maximum Efficiency
First Aid: The Causes And Treatment Of Confusion
Know What To Do In Case Of Choking With Child Or Adult
Choking Children: What To Do In 5-6 Minutes?
What Is Choking? Causes, Treatment, And Prevention
Respiratory Disobstruction Manoeuvres – Anti-Suffocation In Infants
Resuscitation Manoeuvres: Cardiac Massage On Children
The 5 Basic Steps Of CPR: How To Perform Resuscitation On Adults, Children And Infants