
Treatment and therapy of gallstones
Most gallstones are asymptomatic and are often diagnosed by chance, perhaps during an ultrasound performed for other reasons
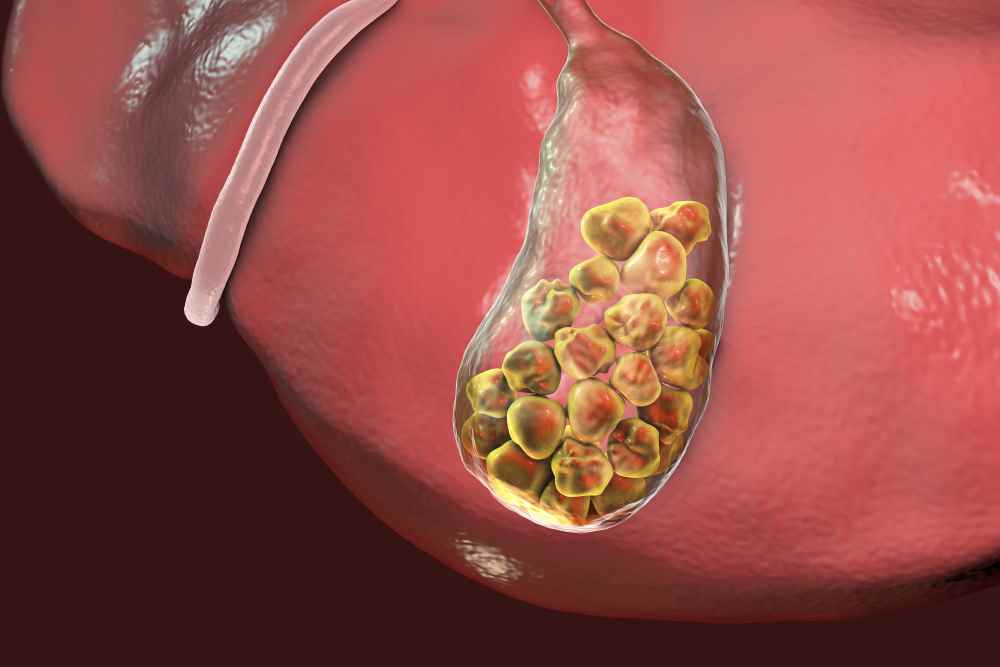
To become symptomatic, the stone must obstruct a visceral structure, for example, the cystic duct.
Only 20 to 30% of patients with asymptomatic calcinosis develop symptoms within 20 years.
Since about 1% of asymptomatic patients have stone complications before the onset of symptoms, prophylactic cholecystectomy is not justified in asymptomatic patients, indeed some say it may worsen functional disorders in patients with IBS.
The numerous biliary colics and frequent consequent inflammation can lead not only to acute cholecystitis (with absolute indication for cholecystectomy) but also to chronic cholecystitis with all possible sequelae.
How to treat gallstones?
Cholecystectomy is the therapy of choice in patients with symptomatic gallstones and reasonable anesthesiologic risk.
It can be performed laparotomically or laparoscopically.
In the former case, the entire gallbladder with all its contents is removed through a laparotomic opening of the abdomen; it is a low-risk surgery with a near-zero intraoperative mortality (risk factors are advanced age, presence of obstruction with exploration of the choledochal duct, and the need for emergency rather than elective surgery).
Laparoscopic cholecystectomy was introduced into routine practice in the late 1980s and consists of a closed-abdomen operation, with the aid of certain instruments (video camera, operating tools) that are inserted into the abdomen and allow the removal of the cholecyst and its contents.
The advantages are related to shorter hospital stay (patients are usually discharged 24 hours after the procedure), reduced pain in the postoperative period, and shorter convalescence time.
Complications of the procedure are fairly overlapping with those of traditional surgery, as is mortality.
In a certain proportion of patients (about 5%), laparoscopic cholecystectomy is found to be impossible and is converted to traditional open abdomen cholecystectomy during the same operating session.
Contraindications to laparoscopic cholecystectomy are respiratory failure from pulmonary emphysema, recent myocardial infarction, decompensated liver cirrhosis, marked degree obesity, previous abdominal surgery for possible intraabdominal adhesions.
In the case of choledochal stones, treatment may be endoscopic or surgical
Sometimes it is necessary to investigate the diagnosis preoperatively with cholangiography (also intraoperatively if necessary) or with MRI cholangiopancreatography, if lithiasic remnants are suspected in the intra- or extra-biliary tree or problems inherent in Vater’s papilla, Oddi’s sphincter, and pancreatic ducts, which are dangerous for the onset of possible pancreatitis.

Today, then, Robotics is becoming more and more established and widespread, in particularly well-equipped centers with trained and experienced personnel, even in that field of surgery, and for particular situations.
Pharmacological treatment of gallstones, when is it possible?
Medical treatment of gallstones by drugs such as cheno and ursodesoxycholic acids, which act by solubilizing biliary cholesterol and reducing its hepatic synthesis and also its intestinal absorption, is possible.
In about 30-40% of patients with small (size less than 10 mm), pure cholesterol, radiolucent (i.e., with minimal calcium) stones and with a normofunctioning gallbladder, stone dissolution can be achieved.
The problem is that such treatment must be protracted for long periods (years).
Not only that: dissolution occurs in about 70% of ideal subjects with 1 year of therapy, but in 60% of patients with benefit there is recurrence after 10 years.
Shock waves generated outside the body by special devices can shatter gallstones, in the same way as for kidney stones.
Inclusion criteria for this treatment are verifiable, however, in only one-fifth of patients with gallstones, and such therapy can frequently result in biliary colic and other major complications.
Read Also:
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
Kidney Stones: How They Form And How To Avoid Them
Renal Colic, How Does It Manifest Itself?
Biliary Colic: How To Recognise And Treat It
Intestinal Obstruction: What Is Faecaloid Vomiting?