
Structural deformities of the spine: scoliosis
Scoliosis is an abnormal curvature of the spine that occurs during an individual’s growth in the period before puberty
Most cases of scoliosis are mild, but some spinal deformities worsen as the child grows so much that they can develop into a disabling disorder over time.
A particularly pronounced spinal curve can reduce the amount of space within the chest, making it difficult for the respiratory system to function properly.
Children with mild scoliosis are monitored closely, usually with serial X-rays, for any worsening. In many cases, no treatment is necessary.
Some children will need to wear a brace to prevent the curve from worsening, while others may need surgery to prevent the scoliosis from causing problems to the internal organs.
Scoliosis, what is it
Scoliosis is a structural deformity of the spine, which twists in three planes:
- on the frontal plane it manifests itself with lateral bending,
- on the sagittal plane it manifests itself with an alteration of the curves,
- on the axial plane it manifests itself with a rotation.
Scoliosis generally occurs during growth, worsening as the bones mature.
The growth peak occurs at the beginning of puberty.
If the deformity is sufficiently accentuated, its evolution does not end with growth: a scoliosis over 30°, and even more frequently one over 50°, grows by about 1° per year even when the patient is an adult.
Scoliosis, causes and complications
To date, an unambiguous cause of scoliosis has not yet been identified.
Experts agree that this disorder is caused, at least in part, by hereditary factors, as it tends to run in families.
Less common types of scoliosis can be caused by
- neuromuscular conditions, such as cerebral palsy or muscular dystrophy,
- congenital defects that affect the development of the bones of the spine,
- injuries or infections of the spine.
The risk factors for developing the most common type of scoliosis are:
- age: signs and symptoms usually begin during the rapid growth that occurs just before puberty,
- gender: although boys and girls have the same risk of developing scoliosis, girls have a much higher risk of worsening the curve and needing treatment,
- family history: scoliosis is sometimes linked to family history, although many cases of scoliosis found in children cannot be traced back to other cases within the family unit.
Most people with scoliosis show a mild form of the condition but, in some patients, this can cause various complications:
- pulmonary and cardiac damage: in severe scoliosis, the rib cage can alter the physiological cardiorespiratory mechanics, making breathing and cardiac contraction more difficult,
- back problems: adults who had scoliosis as children are more likely to develop chronic back pain than people who have never suffered from it,
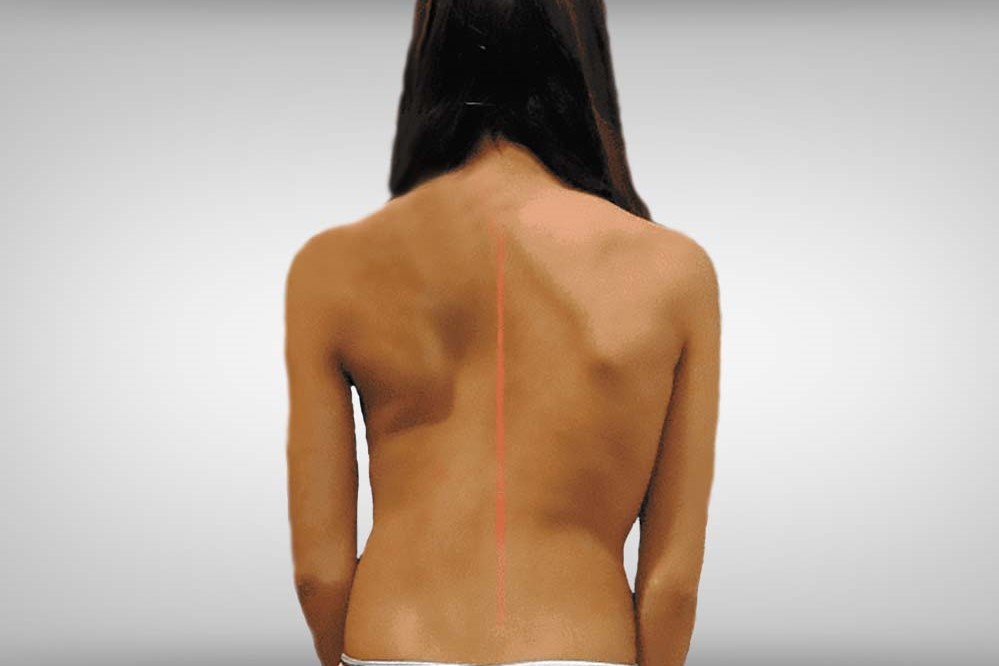
- appearance: when scoliosis worsens, it can cause noticeable changes, including uneven hips and shoulders, prominent ribs and a lateral displacement of the waist and trunk. Individuals with scoliosis often become self-conscious about their appearance, with all the attendant psychological consequences.
Signs and symptoms of scoliosis may include
- uneven shoulder height
- one shoulder blade more prominent than the other,
- waist not parallel to the ground,
- one hip higher than the other.
Scoliosis: diagnosis
The suspicion of scoliosis is confirmed through a physical test, X-ray, CT scan or MRI.
The curve is measured using the Cobb method and is classified in terms of severity according to the degrees of the angle of deformation between the upper and lower somatic limb.
A diagnosis of scoliosis is made when the angle, measured in a posteroanterior X-ray, is greater than 10 degrees.
In general, a curve is considered significant if it is greater than 25-30 degrees.
Curves that exceed 45-50 degrees are considered severe and often require more aggressive treatment.
A standard test that is sometimes used by paediatricians is the Adam’s Forward Bend Test.
During this test, the patient bends forward with feet together and bends 90 degrees at the waist.
From this angle, any asymmetry of the trunk or any abnormal spinal curvature can be detected by the examiner.
This is a simple initial screening test that can detect potential problems, but cannot accurately determine the severity of the deformity.
Imaging tests are required for an accurate and positive diagnosis:
- X-rays: traditional X-rays can show the vertebral structure and the profile of the joints. X-rays of the spine are obtained to search for other potential causes of pain, i.e. infections, fractures, deformities, etc.
- Computed tomography (CT) scan: can show the shape and size of the spinal canal, its contents and the structures around it. Very useful for visualising bone structures.
- Magnetic resonance imaging (MRI): diagnostic test that produces three-dimensional images of body structures, using powerful magnets and dedicated software. It can show the spinal cord, nerve roots and surrounding areas, as well as enlargement, degeneration and deformities. Useful for soft tissue investigation.
Scoliosis in children
Scoliosis in children is classified according to age:
1) Infantile (0 to 3 years),
2) Juvenile (3 to 10 years),
3) Adolescent (11 years and older, or from the onset of puberty until skeletal maturity).
Idiopathic scoliosis comprises the vast majority of cases that occur during adolescence.
Depending on its severity and the age of the child, scoliosis is managed through careful observation, the use of braces and/or surgery.
In children with congenital scoliosis, there is a known increased incidence of other congenital anomalies.
These are most commonly associated with the spinal cord (20 per cent), the genito-urinary system (20 to 33 per cent) and the heart (10 to 15 per cent).
It is important that evaluation of the neurological, genito-urinary and cardiovascular systems is performed when congenital scoliosis is diagnosed.
Scoliosis in adults
Scoliosis that occurs or is diagnosed in adulthood is different from childhood scoliosis, as the underlying causes and treatment goals differ in patients who have already reached skeletal maturity.
Most adults with scoliosis can be divided into the following categories
- adult patients with scoliosis who were treated surgically when they were teenagers,
- adults who did not receive treatment when they were younger,
- adults with a type of scoliosis called degenerative scoliosis.
Degenerative scoliosis most frequently occurs in the lumbar spine (lower back) and most commonly affects people aged 65 years or older.

It is often accompanied by spinal stenosis or narrowing of the spinal canal, which irritates the nerve roots, disrupting their normal functioning.
The back pain associated with degenerative scoliosis usually starts gradually and is related to activity.
The curvature of the spine in this form of scoliosis is often minor, so surgery is only recommended when conservative methods fail to alleviate the pain associated with the condition.
What treatments are effective in combating scoliosis
Most children suffer from mild scoliosis and will probably not need treatment involving a brace or surgery.
Patients with mild scoliosis are monitored for changes in the degree of curvature as they grow.
Although guidelines exist for the management of mild, moderate and severe scioliotic curves, the decision to initiate treatment is always made on an individual basis, in consultation with the patient.
Factors to consider include:
- gender: girls have a much higher risk of progression than boys,
- severity of the curve: more severe curves are more likely to worsen over time,
- type of curve: double curves, also known as S-shaped curves, tend to worsen more often than C-shaped curves,
- position of the curve: curves located in the middle (thoracic) section of the spine worsen more often than curves in the upper or lower sections of the spine,
- growth: if a child’s bones have stopped growing, the risk of curve progression is low. This also means that the brace has more effect in children whose bones are still growing.
Scoliosis brace
If the child’s bones are still growing and he or she suffers from moderate scoliosis, the doctor may recommend the use of a brace.
Wearing a brace will not cure the scoliosis or reverse the curve, but it will usually prevent further progression of the deformity.
The most common type of brace is made of plastic and is shaped to fit the body and is almost invisible under clothing.
The effectiveness of a brace increases with the number of hours per day during which it is worn.
Children wearing braces can usually participate in most activities and have few limitations.
If necessary, they can remove the brace for sports or other physical activities.
The brace is removed when the bones stop growing.
Scoliosis surgery
Severe scoliosis usually progresses over time, so the doctor may suggest surgery to reduce the severity of the spinal curve and to prevent it from getting worse.
The most common type of surgery for scoliosis is spinal fusion (or spinal arthrodesis).
In spinal fusion, surgeons connect two or more vertebrae so that they cannot move independently.
Pieces of bone or a material with similar characteristics are placed between the vertebrae
Metal rods, hooks, screws or wires generally hold that portion of the spine in a certain position while the old and new bone material fuse together.
If scoliosis progresses rapidly at a young age, surgeons can install a rigid rod that is adjustable in length to accommodate the child’s growth.
This rod is fixed at the upper and lower portions of the spinal curvature and is usually lengthened every six months.
Complications of spinal surgery may include bleeding, infection, pain or nerve damage.
Rarely, the bone fails to heal and further surgery may be necessary.
Although physical therapy exercises cannot stop the progression or reverse scoliosis, exercise can improve overall health and well-being.
The effects of scoliosis on the patient’s life
Dealing with scoliosis is difficult for a young person at an already complicated stage of life.
Adolescents face physical changes as well as emotional and social challenges.
With the diagnosis of scoliosis, difficult emotions such as anger, insecurity and fear can arise.
A strong and supportive peer group can have a significant impact on a child’s or adolescent’s acceptance of scoliosis, guardianship or surgical treatment.
It is therefore important for a parent to encourage their child to talk to their friends and ask for their support.
Parents should consider joining a support group for parents and children with scoliosis.
Support group members can provide advice, pass on real-life experiences and help the person get in touch with other people facing similar challenges.
Read Also
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
Is Correcting Scoliosis Possible? Early Diagnosis Makes All The Difference
What Is The Full-Spine Radiography And What Is It For?
How To Survive The Witch’s Stroke: Discovering Acute Low Back Pain
Lumbago: What It Is And How To Treat It
Back Pain: The Importance Of Postural Rehabilitation
Epiphysiolysis: ‘Train Paediatricians To Avoid Late Diagnoses’
Idiopathic Scoliosis: What It Is And How To Treat It
Diagnosis And Treatment For Adult Scoliosis
Scoliosis And Hyperkyphosis: From Adolescence To Adulthood